Creatine for neurological rehabilitation: Could it have value as a supplement?
Creatine monohydrate is the most studied supplement in sport, with a safety record few products can match. From time to time, someone living with a spinal cord injury, or a therapist working with neurological clients, asks me about it: if it builds muscle and improves performance in athletes, would it help someone rebuilding strength after a neurological injury? It is an interesting question.
This article works through what the research shows, its limitations, and what that means in practice. The short version is that the evidence in healthy and older adults is strong, the evidence in neurological rehabilitation is thin and mixed.
One point before we begin. Creatine is a food supplement, not a medicine, and nothing here is individual medical advice. If you have kidney problems, take other medication, or have a complex medical picture, speak to your doctor or a dietitian before starting anything. With that said, let us look at the evidence.
The starting point:

There is no doubt that creatine works in healthy people who train. Taken alongside resistance training, typically 5 to 10 grams a day across several weeks, creatine reliably increases muscle mass, strength, and exercise capacity, and it amplifies the muscle-building response to training. A meta-analysis in older adults found roughly 1.4 kilograms more lean tissue in those taking creatine and doing resistance training than in those training alone. The International Society of Sports Nutrition, which has published the most thorough position statement on the subject, treats these effects as well established.
One detail in that evidence matters more than any other for our community, and it is easy to miss. Creatine's benefit depends on the muscle being loaded. It is not a substance you swallow that magically thickens muscle on its own. It works by helping a muscle do more work during training, so the training drives the adaptation, and creatine enlarges the result. Take away the training, and you take away most of the effect.
What happens in neurological populations
The robust evidence supporting the use of creatine comes from athletes and healthy older adults engaged in voluntary resistance training. The use of creatine following a neurological injury has much less evidence: just a handful of small studies that do not point in the same direction.
Spinal cord injury: a genuine but narrow positive signal
The most relevant study for our readers is also one of the oldest. Jacobs and colleagues, working at the University of Miami in 2002, ran a randomised, double-blind, placebo-controlled crossover trial in sixteen men with complete cervical-level spinal cord injury (C5 to C7). After 7 days of 20 g/day of creatine, the participants showed significantly greater peak oxygen uptake and a higher ventilatory anaerobic threshold during arm exercise than on placebo. In plain terms, their upper-body exercise capacity improved.
That is a real finding, and it is why creatine continues to appear in the SCI literature. It carries two qualifications. It was a small, short, acute study of exercise capacity, not a long study of everyday function, and not every measure improved. The value lies in showing that creatine can be useful in tetraplegia, not in proving a functional transformation.
A later pilot adds a little on the muscle side. A 2018 study followed fourteen people with SCI through eight weeks of upper-body resistance training. Those taking a modest 3 grams of creatine per day showed a significant improvement in corrected arm muscle area compared with controls, although strength gains were significant only within the creatine group, not relative to controls. It is a small, hypothesis-generating study, and, once again, it pairs creatine with training.
Stroke: a careful trial that found nothing
The most rigorous neurological trial to date is recent. The ICaRUS Stroke Trial, published in Nutrients in 2024, gave thirty older adults with acute ischaemic stroke either creatine (10 grams twice daily) or placebo for seven days in hospital. Both groups also received protein supplementation and daily mobility training. Creatine made no difference to functional capacity, muscle strength, muscle mass, or muscle breakdown, either at seven days or at the ninety-day follow-up. There was one intriguing biochemical signal: a fall in the protein progranulin, but no measured functional benefit.
Multiple sclerosis: also negative
The evidence on multiple sclerosis tells a similar story. Malin and colleagues conducted a 14-day double-blind crossover trial in 11 people with MS. Creatine did not improve muscle work, muscle power, or habitual fatigue. Fatigue is one of the most disabling symptoms in MS, so this was a sensible thing to test, and the answer, on this small trial, was no. As fatigue can be minimised by using tactics that directly stimulate muscle groups, such as FES Cycling (thereby avoiding centrally mediated fatigue), it would be interesting to investigate whether better results could be achieved.
Disuse and immobilisation
You may have read that creatine protects muscle during immobilisation and speeds rehabilitation afterwards. The source of that idea is a study by Hespel and colleagues in 2001, in which creatine taken during two weeks of leg casting and ten weeks of rehabilitation was associated with greater regrowth of muscle fibre size and strength than placebo, alongside changes in a muscle-regulating factor called MRF4. It is a mechanistically interesting result, but it was a study in healthy volunteers in whom the immobilised limb was then actively rehabilitated. It is encouraging for the rehabilitation idea in general, but it is not evidence from a neurological population, and the stronger versions of the claim circulating online overstate it.
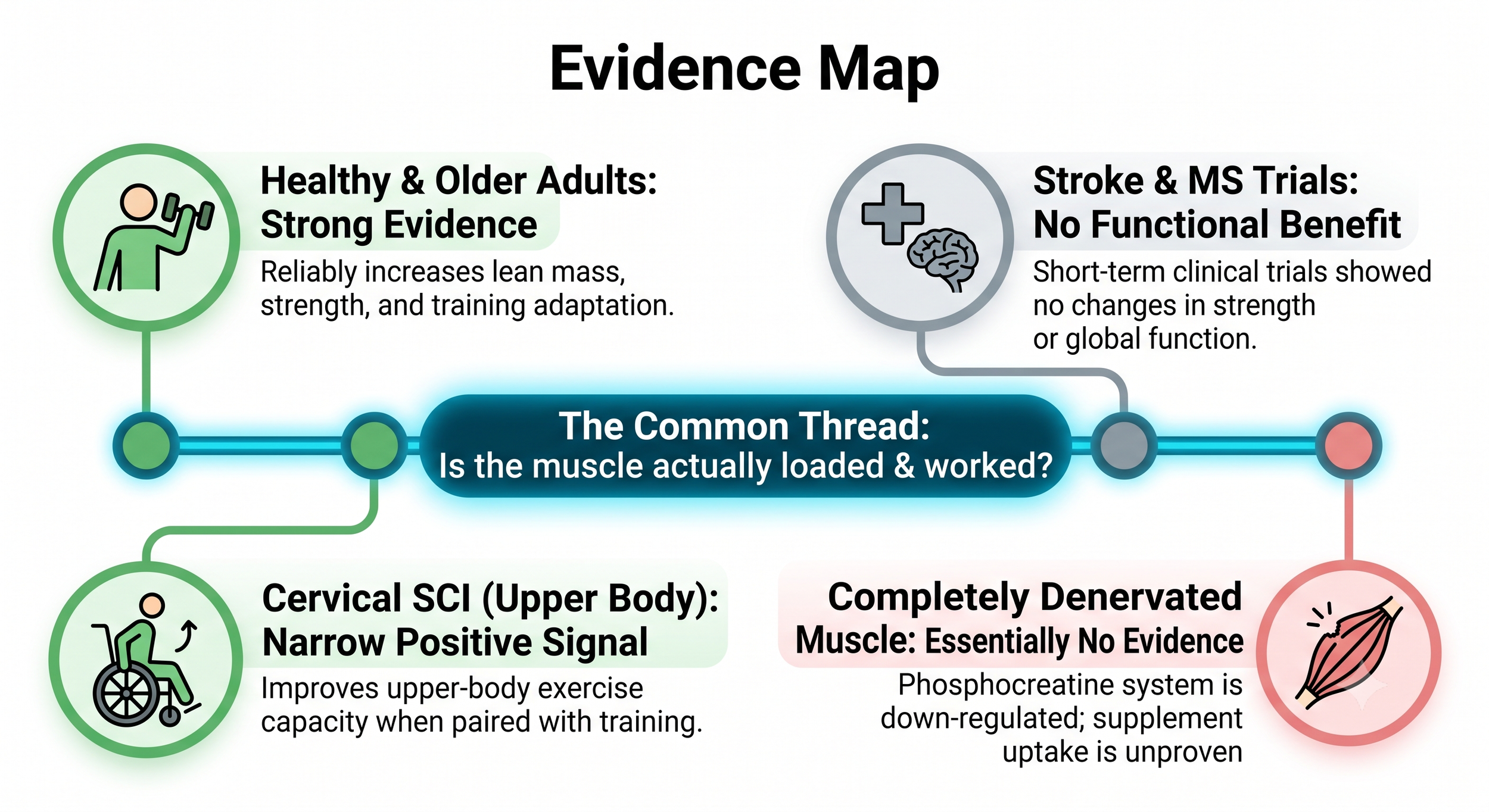
The pattern across all of this is consistent. Where the muscle can be loaded and trained, whether in athletes, older adults, recovering limbs, or the arms of people with tetraplegia, creatine has something to offer. Where the trials were short, the muscle was weak or inactive, or the outcome was global function rather than trained capacity, the benefit disappears.
Is it safe for someone with a neurological condition?
Safety is an important issue, obviously, and sometimes people have heard the most alarming things, mostly about kidneys.
For the general population, the safety record is reassuring and long. The ISSN position concludes that both short- and long-term creatine use, at doses up to 30 grams a day for as long as five years, is safe and well tolerated, and that there is no compelling evidence that it harms kidney function in healthy or indeed clinical populations. The only consistently reported side effect is a small gain in body weight, largely water held inside the muscle. A 2025 meta-analysis focused on the kidneys found only a small increase in serum creatinine, a marker that rises simply because creatine breaks down into creatinine, with no meaningful change in the kidneys' filtration rate. The rise reflects the supplement's chemistry, not damage.
There is an important caveat for our readers specifically. Those reassuring kidney studies deliberately excluded people with kidney disease, neurological conditions, and spinal cord injury. So general population safety data does not automatically translate to someone with a neurogenic bladder, reduced mobility, or borderline kidney function. The ICaRUS stroke trial gives a practical illustration: three people taking creatine had a temporary rise in serum creatinine that resolved quickly once they were given fluids, and three had some diarrhoea. None of it was judged to be caused by the creatine, but it makes the sensible precaution obvious.
For anyone living with a neurological condition, the best precaution is hydration. If you manage your fluids carefully because of a neurogenic bladder, are prone to dehydration, or have kidney function that is not entirely normal, creatine is a conversation to have with your doctor before you start, not a decision to make based on a supplement website. Stomach upset, when it happens, is usually mild, tied to larger single doses, and easily avoided by splitting the dose. The weight gain is real but small and worth knowing about if you self-transfer or if your weight margins matter.
What about cognition and brain fog?
There is one more question worth raising, because cognitive fatigue and what many people call brain fog are among the most wearing parts of life after a neurological injury. Creatine fuels the brain much as it fuels muscle, so it is reasonable to ask whether it helps the mind as well as the body.
From the start, I should say that in spinal cord injury, stroke, and multiple sclerosis specifically, this has barely been studied. I could find no trials of creatine and cognition in these populations. So anything said here is an extension of other groups, not direct evidence in ours.
That said, the wider picture is mildly encouraging. A 2024 meta-analysis of 16 trials found that creatine produced small but measurable improvements in memory, attention, and information-processing speed, with the effect tending to be larger in people with underlying illness and in older adults. A separate review of memory studies found the clearest benefit in adults aged 66 to 76. The pattern is that creatine seems to help most when the brain's energy supply is under strain, for example, during sleep deprivation, ageing, general stress or certain medical conditions.
The area with the most rehabilitation-relevant interest is traumatic brain injury and concussion, where creatine is being actively investigated as a protective adjunct, although the evidence there is still early.
The benefits seen in healthy and older adults are modest, not dramatic. And raising creatine levels in the brain is harder and slower than raising them in muscle, which is the same uptake problem we meet again below, in a different organ. So creatine is a plausible, low-risk thing to consider if cognitive fatigue is a problem, but it is a reasonable hypothesis rather than a proven treatment, and nobody should expect it to clear brain fog on its own.
How it works, and why the muscle has to do something
We've said a lot up to now without actually explaining how creatine works. To understand why creatine helps trained muscle but not inactive muscle, it helps to know what it actually does.
In simple terms, creatine is like a small “extra battery” or rocket fuel for your muscles, helping them produce quick bursts of energy. Creatine appears to make strength training a bit more effective.
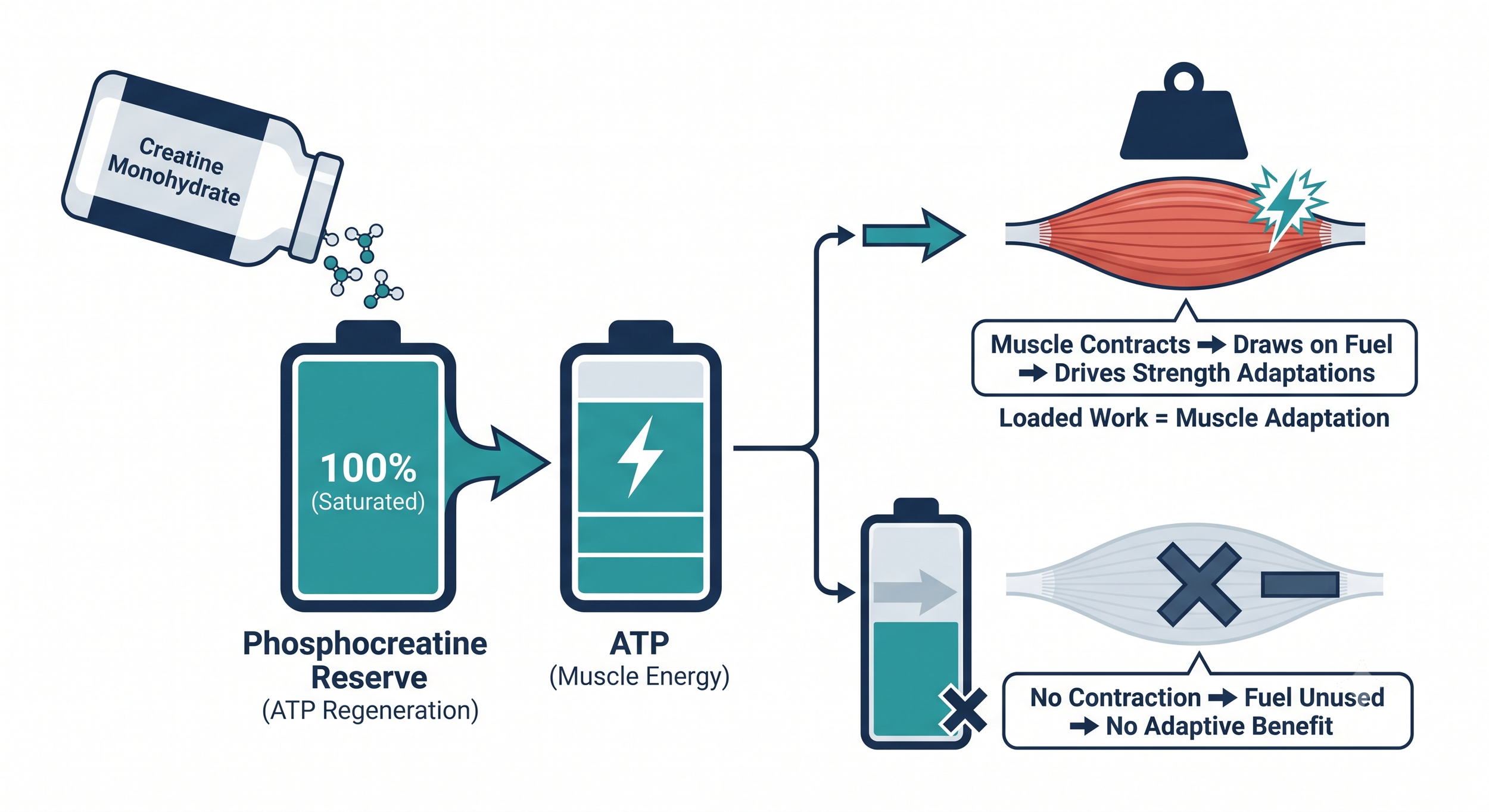
Muscle runs on a molecule called ATP, but it stores only a few seconds' worth, which is rapidly exhausted. During short, hard efforts, it rapidly regenerates ATP from a reserve called phosphocreatine via the creatine-kinase energy shuttle. Supplementing with creatine increases the amount of phosphocreatine stored in muscle, which means faster ATP regeneration and a little more high-intensity work before fatigue onset. That extra work, repeated across a regular training programme, is what eventually produces more muscle and more strength.
The key point is in that chain. Creatine "fills the fuel tank". The muscle still has to "drive the car". If the muscle is not contracting hard against a load, the larger fuel reserve is not deployed.
the creatine “fuel tank”
This is exactly where the question becomes interesting for our field and genuinely unresolved.
What about a muscle that cannot contract voluntarily because the nervous system no longer commands it?
Two cautions are needed.
The first concerns denervated muscle, where the lower motor neuron itself is damaged and the muscle has lost its nerve supply. The evidence is almost absent. There is a single rat study by Ozkan and colleagues in 2005 in which oral creatine improved recovery of denervated hind-limb muscle while the nerve was regrowing. That is one animal study about muscle being reinnervated, not muscle that is permanently denervated, and it should not be stretched further than that. We do not have human evidence that creatine helps denervated muscle, and there are good biological reasons for caution.
The second caution concerns uptake. Getting creatine into muscle is not guaranteed. Chronically weakened and wasted muscle, as seen after long-standing spinal cord injury, may result in poor creatine uptake, and no human study has yet confirmed that intramuscular creatine actually rises in paralysed muscle. So with the population we most want to help, we cannot even be sure the supplement reaches its target in useful amounts.
KEY POINT: creatine works through trained, contracting muscle. The more a muscle can be activated and loaded, the more plausible a benefit becomes. The less it can be activated, the weaker the rationale, until in fully denervated muscle the case more or less disappears on current evidence.
That principle leads to a thought that sits close to the work we do. Much of what Anatomical Concepts provides, from functional electrical stimulation for paralysed but innervated muscle to specialised stimulation for denervated muscle, exists to make muscle contract and work when the nervous system no longer drives it voluntarily. FES cycling, in particular, produces exactly the repeated, loaded muscle activity that creatine's mechanism depends on. Whether creatine combined with that kind of stimulation training produces a measurable benefit is, as far as I can find, untested. It is one of the more sensible research questions in this area, and it is precisely the combination that the short, sedentary trials never examined. I would say it is the version of the question most worth asking.
A closer look at complete denervation
It helps to separate two situations that often get lumped together. Most spinal cord injuries are upper motor neuron lesions: the muscle keeps its own nerve supply and can still be made to contract, by reflex, by whatever voluntary pathway survives, or by ordinary neuromuscular electrical stimulation (NMES). Every creatine study in spinal cord injury, including the work in tetraplegia, was done in muscle of this kind. Complete denervation is a different problem. When the lower motor neuron itself is lost, as in a cauda equina or conus lesion or a peripheral nerve injury, the muscle has no nerve supply at all, and that changes the picture for creatine specifically, not merely in general.
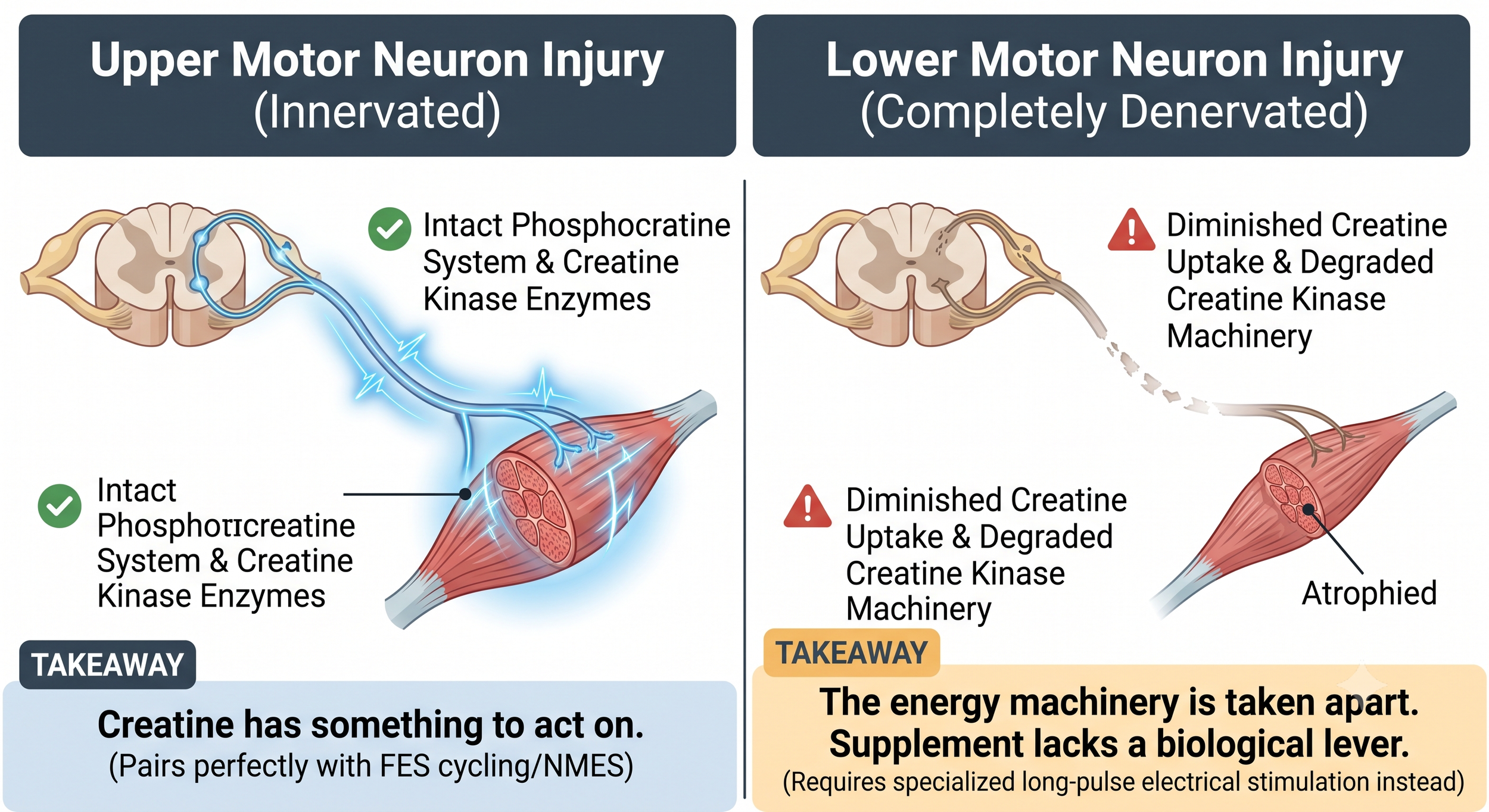
Two findings explain why, and both go deeper than the muscle simply not being trained. First, denervation runs down the phosphocreatine system that creatine acts on. In classic animal work, denervation lowered the muscle's creatine phosphate content and reduced the rate at which it took up creatine, so the cell becomes worse at importing creatine at the very moment we would want to load it. Second, chronic denervation reduces muscle creatine kinase, the enzyme that drives the phosphocreatine shuttle, with reinnervation restoring it. Denervation does not leave the energy system idle; it takes part of it apart.
The consequence is straightforward. If both creatine uptake and the creatine kinase machinery are diminished, then there is less for rationale for swallowing more creatine. A rationale that is already thin for paralysed but innervated muscle becomes thinner still where there is no nerve supply at all.
None of this means denervated muscle cannot be helped. It means the effective lever is not a supplement. Completely denervated muscle does not respond to conventional FES, because there is no nerve to excite; it requires the specialised long-pulse stimulation developed for this exact situation, the principle behind dedicated denervated-muscle systems. That approach has a real evidence base for rebuilding muscle bulk and force, and the encouraging finding from the Vienna work is that muscle can be trained even 15 to 20 years after denervation, although full rebuilding takes years of consistent stimulation. Creatine has no comparable evidence here. The only version of the creatine question that makes biological sense in denervated muscle is whether it adds anything on top of stimulation that is already making the muscle work, and even then the uptake problem may have the final say.
Practical dosing, for those who decide to try it
If, after discussing it with your doctor, you decide that creatine is worth a trial, the protocol is simple and the same as that used in the research.
There are many brands and formulations offered as creatine. You ideally want a premium brand of micronised creatine monohydrate with nothing added. The gold standard for premium creatine is "Creapure" grade. It uses a different, cleaner manufacturing process that results in fewer contaminants (including heavy metals and dehydrotriazine).
There are two ways to "fill" the muscle. The "traditional" way is a loading phase: roughly 5 grams, four times a day, for five to seven days, which saturates the muscle quickly. The slower way is to skip loading and take 5 grams a day for about a month, which reaches the same end result without the larger early doses. For most people in rehabilitation who are not chasing a competition date, a lower, steady dose is perfectly reasonable and gentler on the stomach. After that, a maintenance dose of 3 to 5 grams a day keeps the muscle topped up.
A few practical notes. Plain creatine monohydrate is the form with all the evidence behind it; the micronised version is simply ground finer so it mixes more easily, and it is a sensible choice, but it is not a different or superior compound. Timing matters very little, so take it whenever you remember it consistently, which is what actually predicts whether it works. Adequate fluid intake matters for the reasons given above.
One realistic expectation to set: not everyone responds, and people with spinal cord injury may be among the less likely to, for the uptake reasons already described. If you try it, give it a fair trial of several weeks alongside whatever training or stimulation you are doing, and judge it on whether your trained capacity actually improves.
Where this leaves us
In healthy and older adults who train, creatine works. In cervical spinal cord injury, a small but real body of evidence suggests it can improve upper-body exercise capacity and possibly muscle size when paired with training. In stroke and multiple sclerosis, the careful trials we have, admittedly small, did not show a benefit. For denervated muscle, the evidence is essentially a single animal study and should not be relied upon. For cognition, the general signal is mildly positive but has not been tested in our populations.
Throughout the studies, the benefit is linked to one thing: whether the tissue is being actively worked.
In terms of safety, creatine is one of the better-studied supplements, and for most people, it is well tolerated. The qualification for our community is real but manageable: reassuring kidney data excluded people like our clients, so hydration and a prior conversation with a doctor are sensible precautions, particularly for a neurogenic bladder or any kidney concern.
My own reading is that creatine is a low-cost, low-risk adjunct that makes the most sense for the person who can train, including the person using electrical stimulation to make their muscles train. It is not a treatment for paralysis, it is not a substitute for doing the work, and it is not a reason for hope on its own. Used alongside a genuine training stimulus, in someone without a specific medical reason to avoid it, it is a reasonable thing to try with clear eyes.
Where to go from here
If you are considering creatine as part of a rehabilitation programme, two questions are worth answering first. Can the muscle you want to help actually be loaded and worked, whether voluntarily or through stimulation? And is there any medical reason, kidney function, fluid management, or other medication to check with your doctor before starting? If the muscle can be trained and there is no medical flag, a careful trial carries little downside.
At Anatomical Concepts our role is to help people get the most from the right rehabilitation technology, assessed and set up for the individual rather than sold off the shelf. We cannot give individual medical advice on supplements, but if you are weighing up how something like creatine might fit alongside a stimulation or FES programme, we are happy to help you think it through clearly, including where it does not fit.
The evidence does not allow anyone to promise that creatine will help after a neurological injury. It does let us say something more useful: it is most likely to help the tissue you are actually training, which is exactly the tissue our stimulation technology is designed to wake up.
Further reading
Kreider RB, Kalman DS, Antonio J, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition 2017;14:18. https://doi.org/10.1186/s12970-017-0173-z
Antonio J, Candow DG, Forbes SC, et al. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? Journal of the International Society of Sports Nutrition 2021;18(1):13. https://doi.org/10.1186/s12970-021-00412-w
Jacobs PL, Mahoney ET, Cohn KA, Sheradsky LF, Green BA. Oral creatine supplementation enhances upper extremity work capacity in persons with cervical-level spinal cord injury. Archives of Physical Medicine and Rehabilitation 2002;83(1):19-23. https://doi.org/10.1053/apmr.2002.26829
Amorim S, Teixeira VH, Corredeira R, et al. Creatine or vitamin D supplementation in individuals with a spinal cord injury undergoing resistance training: a double-blinded, randomized pilot trial. Journal of Spinal Cord Medicine 2018. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6055973/
Souza JT, Minicucci MF, Ferreira NC, et al. Influence of Creatine Supplementation on Muscle Mass and Strength After Stroke (ICaRUS Stroke Trial): a randomized controlled trial. Nutrients 2024;16(23):4148. https://doi.org/10.3390/nu16234148
Malin SK, Cotugna N, Fang CS. Effect of creatine supplementation on muscle capacity in individuals with multiple sclerosis. Journal of Dietary Supplements 2008;5(1):20-32. https://doi.org/10.1080/19390210802328974
Hespel P, Op't Eijnde B, Van Leemputte M, et al. Oral creatine supplementation facilitates the rehabilitation of disuse atrophy and alters the expression of muscle myogenic factors in humans. Journal of Physiology 2001;536(Pt 2):625-633. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2278864/
Ozkan S, et al. Effect of systemic creatine monohydrate supplementation on denervated muscle during reinnervation: experimental study in the rat. Journal of Reconstructive Microsurgery 2005;21(8):573-579. https://pubmed.ncbi.nlm.nih.gov/16292735/
Hofmann WW, Butte J, Leon HA. Relationship of intracellular creatine concentration and uptake to muscle mass in vivo. American Journal of Physiology 1978;235(5):C199-203. https://doi.org/10.1152/ajpcell.1978.235.5.C199
Washabaugh CH, Ontell MP, Kant JA, et al. Effect of chronic denervation and denervation-reinnervation on cytoplasmic creatine kinase transcript accumulation. Journal of Neurobiology 2001;47(3):194-206. https://doi.org/10.1002/neu.1027
Kern H, Hofer C, Mödlin M, et al. Denervated muscles in humans: limitations and problems of currently used functional electrical stimulation training protocols. Artificial Organs 2002;26(3):216-218. https://doi.org/10.1046/j.1525-1594.2002.06933.x
Hultman E, Söderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. Journal of Applied Physiology 1996;81(1):232-237. https://pubmed.ncbi.nlm.nih.gov/8828669/
Xu C, Bi S, Zhang W, Luo L. The effects of creatine supplementation on cognitive function in adults: a systematic review and meta-analysis. Frontiers in Nutrition 2024;11:1424972. https://doi.org/10.3389/fnut.2024.1424972
Prokopidis K, Giannos P, Triantafyllidis KK, et al. Effects of creatine supplementation on memory in healthy individuals: a systematic review and meta-analysis of randomized controlled trials. Nutrition Reviews 2023;81(4):416-427. https://doi.org/10.1093/nutrit/nuac064
Roschel H, Gualano B, Ostojic SM, Rawson ES. Creatine supplementation and brain health. Nutrients 2021;13(2):586. https://doi.org/10.3390/nu13020586
Candow DG, Forbes SC, Ostojic SM, et al. "Heads Up" for creatine supplementation and its potential applications for brain health and function. Sports Medicine 2023;53(Suppl 1):49-65. https://doi.org/10.1007/s40279-023-01870-9
Images generated with AI