Articles
Filter by Topic
- Adaptive Sport 2
- Artificial Intelligence 1
- Bike Labyrinth 3
- Bone density 1
- Brachial Plexus 2
- Bridging the Gap 1
- Bridging the Gap 1
- Carbonhand 4
- Cardiovascular 1
- Cauda Equina Syndrome 1
- Client Stories 4
- Cognition 1
- Company Updates 3
- Decision Making 2
- Dementia 1
- Denervation 28
- Diabetic Foot 12
- Efficiency 1
- Electrotherapy 32
- Exercise Benefits 34
- FES Cycling 22
- Fatigue 1
- Functional Electrical Stimulation (FES) 64
- Gait 2
- Goal Setting 5
- Grip 3
- Guidelines 1
- HRV 1
- Healthspan 2
- Indego 13
- Lifestyle 10
- Lower Motor Neuron 1
- Mobility 17
- Motivation 2
- NMES 3
- Nerve injury 3
- NexStride 1
- Occupational Therapy 1
- Orthotic 15
- PRAFO 29
- Pain 7
- Parkinsons 2
- Pressure Ulcers 16
- Product Updates 7
- RISE Stimulator 13
- Safety 2
- Spasticity 3
- Sponsor 1
- Standing 5
- Stim2Go 9
Article Length
- 1 minute read 3
- 10 minute read 23
- 11 minute read 4
- 12 minute read 10
- 15 minute read 13
- 18 minute read 1
- 2 minute read 4
- 24 minute read 1
- 25 minute read 1
- 26 minute read 1
- 28 minute read 1
- 3 minutes read 9
- 4 minute read 34
- 5 Minute read 17
- 6 minute read 6
- 7 minute read 17
- 8 minute read 12
- 9 minute read 3
- FES 2
- FoG 1
- Long Read 1
- PRAFO 1
- Seven Minute Read 1
- awareness 1
- carbonhand 2
- cognitive 1
- cues 1
- freezing gait 1
- freezing of gait 1
- gait 1
- neurological 1
- neuroplasticity 1
- nexstride 2
- occupational therapy 1
- occupational therapy day 1
- orthopaedics 1
- orthotic 1
- parkinson's 1
- pressure 1
- pressure relief 1
- prevention 1
- rehabilitation 2
- stroke 1
- ulcers 1
- world stroke day 1

What a Nerve Conduction Study Actually Tells You, and Why It Matters Before Electrical Stimulation
If you have a nerve injury, whether at the spine or further out in a limb, at some point, someone may send you for a nerve conduction study. You will lie on a couch while a neurophysiologist delivers small electrical pulses to your skin and, a little later, puts a fine needle into one or two muscles. A few weeks after that, a report lands with your consultant. It is dense, full of numbers and abbreviations, and it is written for one clinician to read to another. Almost nobody explains it to the person whose nerve it describes. Just this morning, I read a note from a client who said, "I had a nerve conduction test, which indicated severe injury to the nerves." You might wonder, like me, what severe means, and what do I do about it?
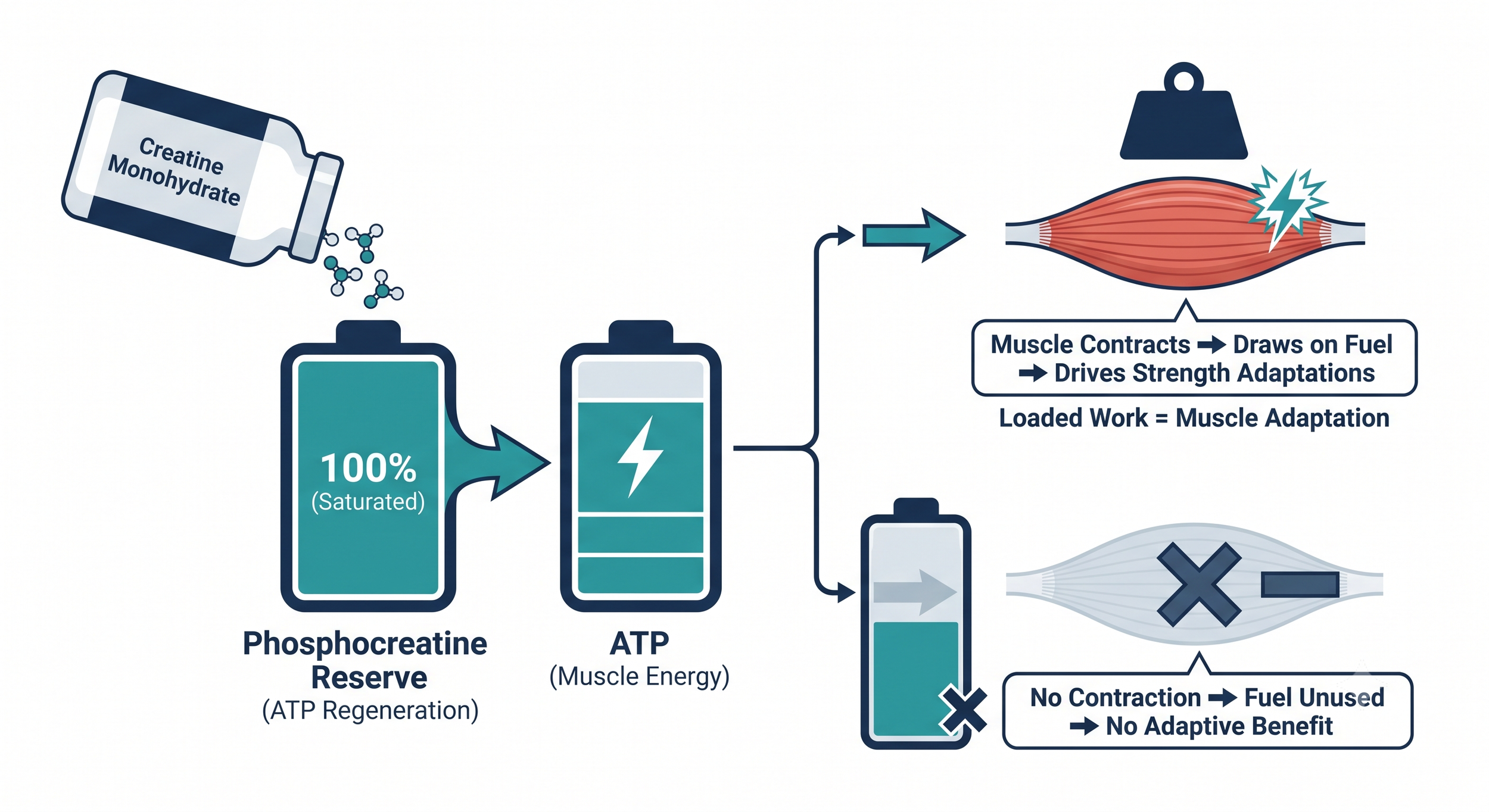
Creatine for neurological rehabilitation: Could it have value as a supplement?
Creatine monohydrate is the most studied supplement in sport, with a safety record few products can match. From time to time, someone living with a spinal cord injury, or a therapist working with neurological clients, asks me about it: if it builds muscle and improves performance in athletes, would it help someone rebuilding strength after a neurological injury? It is an interesting question.
This article works through what the research shows, its limitations, and what that means in practice. The short version is that the evidence in healthy and older adults is strong, the evidence in neurological rehabilitation is thin and mixed.
One point before we begin. Creatine is a food supplement, not a medicine, and nothing here is individual medical advice. If you have kidney problems, take other medication, or have a complex medical picture, speak to your doctor or a dietitian before starting anything. With that said, let us look at the evidence.
When Spasticity Gets in the Way of Standing
For some people, the obstacle to standing up is not weakness. It is the opposite problem: legs that are too stiff, too tense, or too unpredictable to cooperate. You go to move and the leg pushes out straight when you wanted it to bend, or a spasm arrives at the worst possible moment, or simply getting your feet into a sensible position feels like a negotiation. This is spasticity, and for a great many people, after an incomplete spinal cord injury or stroke, it is the single thing standing between them and a useful sit-to-stand.
We have written before about spasticity after spinal cord injury and the limits of medication. This article looks at a more specific question: when spasticity is the thing blocking a functional goal like standing, what can electrical stimulation do about it, and how do the pieces fit together?

One Device, Many Exercises: Getting More From a Single Stimulator
One of the quieter worries in rehabilitation is rarely about the therapy itself. It is about money. Equipment is expensive, budgets are tight, and funding is often uncertain until late in the process. The fear we hear most is not "will this work," but rather "will I spend a significant sum and end up with the wrong thing, or with several things that do not work well together." Does this sound familiar?
It is a reasonable worry, and it deserves a straight answer rather than a sales pitch. This article looks at one practical way of reducing that risk: choosing a single, flexible stimulator that covers several rehabilitation needs, rather than a separate machine for each. The device we have in mind is the Stim2Go, and the point is not so much the brand as the principle behind it.

Standing Up Again: How Responsive Electrical Stimulation Can Support Sit-to-Stand Practice
Ask someone in the early stages of recovery from a spinal cord injury or stroke what they most want to do again, and the answers are often smaller and more specific than you might expect. Not "run a marathon." More often, it is something like rising from a chair without help, managing a transfer to the bed, or pushing up to standing so that getting to the toilet is your own business and nobody else's.
Sit-to-stand sits at the centre of all of that. It is one of the most important movements in daily life and one of the first functional milestones a therapist will work on. If you can move reliably between sitting and standing, a great deal of independence follows. This article looks at how electrical stimulation, and in particular a responsive electrical stimulation device like the Stim2Go, can support sit-to-stand practice as part of a wider rehabilitation programme.

Waveform matters: what new evidence tells us about transcutaneous spinal cord stimulation
Transcutaneous spinal cord stimulation (tSCS) has moved quickly from a research curiosity to a recognised tool in neurological rehabilitation. People living with spinal cord injury, stroke, and multiple sclerosis are asking us about it. Clinicians want to know which device to recommend. Equipment commissioners want evidence-led guidance before authorising spend that can run into tens of thousands of pounds per system.
A paper published in Nature Biomedical Engineering on 12 May 2026 has added something important to that conversation. It is not a clinical trial. It is a careful study of the physics and physiology that govern which nerve fibres a tSCS device actually recruits. The finding is consequential, and it bears directly on the choice of device.
In short: the waveform you choose determines whether tSCS does the thing rehabilitation needs it to do.