Exploring Electrical Stimulation for Pain Relief
Overview
Neuropathic pain is a complex chronic pain condition affecting 7-10% of the global population, arising from damage or disease of the somatosensory nervous system. In this article we examine neuropathic pain mechanisms, conventional treatments, and the role of electrical stimulation as a therapeutic intervention.
In addition to the well-known TENS approaches, we look at the less well-known spinal cord stimulation (SCS) and transcutaneous spinal cord stimulation (tSCS) approaches and their pros and cons.
Definition and Pathophysiology of Neuropathic Pain
Neuropathic pain is defined by the International Association for the Study of Pain as pain caused by a lesion or disease of the somatosensory nervous system.
The somatosensory system refers to the part of the sensory nervous system responsible for processing sensory information from the body. This includes sensations such as touch, temperature, pain, pressure, vibration, and proprioception (the sense of body position and movement). It enables the body to perceive and respond to the physical environment through intricate neural pathways.
Unlike nociceptive pain that results from tissue damage which is often relatively short-lived, neuropathic pain stems from dysfunction within the nervous system itself and can become chronic.
Neuropathic pain presents with characteristic symptoms including burning, shooting, stabbing sensations, electric shock-like pain, "pins and needles" sensations, numbness, and allodynia (pain from normally non-painful stimuli such as brushing or stroking the skin). Patients may experience both continuous and episodic components, with the latter resembling electrical shocks or stabbing sensations.
We often see that neuropathic pain needs to be dealt with as a priority. As it disallows focus on aspects of functional recovery that would otherwise be a first priority for clients.
Underlying Mechanisms
The pathophysiology involves multiple complex changes throughout the nervous system. This beyond the scope of this article but key mechanisms include:
Ectopic impulse generation at sites of nerve injury, including neuromas, dorsal root ganglia, and neighbouring intact afferents
Central sensitisation with increased excitability of spinal dorsal horn neurons
Loss of inhibitory control through reduced GABAergic and glycinergic activity
Neuroimmune interactions involving microglial activation and inflammatory mediator release
Altered gene expression affecting ion channels, neurotransmitter systems, and pain processing pathways
Major Causes of Neuropathic Pain
Peripheral Causes
The most common peripheral causes include:
Diabetes mellitus - responsible for 30% of neuropathic cases and affecting 26% of UK diabetic patients
Post-herpetic neuralgia following herpes zoster infection
Traumatic nerve injuries from accidents or surgical procedures
Cancer-related neuropathy from tumor compression or chemotherapy
Autoimmune conditions such as multiple sclerosis and rheumatoid arthritis
At Anatomical Concepts, as a rehabilitation-focused business, we are mainly dealing with traumatic nerve injuries, which are frequently due to spinal cord injury which accounts for 40% of neuropathic pain cases globally.
Current Treatment Approaches
Treatment follows a tiered, evidence-based approach with multiple therapeutic options.
First-Line Pharmacological Treatments
Gabapentinoids (gabapentin and pregabalin) target voltage-gated calcium channels and represent cornerstone therapy. Clinical trials demonstrate Number Needed to Treat (NNT) values of 7.7 for pregabalin and 6.4 for gabapentin.
Tricyclic antidepressants (amitriptyline, nortriptyline) show the largest effect size in neuropathic pain treatment with NNT of 3.6. They work through multiple mechanisms including serotonin-norepinephrine reuptake inhibition and sodium channel blockade.
Serotonin-norepinephrine reuptake inhibitors (duloxetine, venlafaxine) provide effective pain relief with NNT of 6.4, particularly for diabetic peripheral neuropathy.
Second-Line Treatments
Tramadol and other opioid-like medications
Topical agents including 5% lidocaine and 8% capsaicin patches
Combination therapy using multiple first-line agentsacademic.oup
Third-Line and Advanced Treatments
For refractory cases:
NMDA receptor antagonists (ketamine, dextromethorphan)
Cannabinoids for specific indications
Botulinum toxin type A
Interventional procedures including nerve blocks and neuromodulation
Electrical Stimulation for Neuropathic Pain
Electrical stimulation represents a significant non-pharmacological treatment approach based on the "gate control" theory proposed by Melzack and Wall in 1965. We could debate whether this theory is accurate but nevertheless three main modalities are used clinically:
1. Transcutaneous Electrical Nerve Stimulation (TENS)
TENS applies low-voltage electrical currents through skin surface electrodes, activating large-diameter A-β fibers to inhibit nociceptive transmission.
Mechanisms of Action
TENS operates through multiple pathways:
Peripheral mechanisms including disruption of nociceptive afferent transmission
Spinal segmental effects via the gate control mechanism in the dorsal horn
Supraspinal modulation involving brainstem nuclei and descending inhibitory pathways
Endogenous opioid release with frequency-dependent receptor activation.
Clinical Evidence for TENS
Recent systematic reviews provide moderate-certainty evidence for TENS effectiveness. A comprehensive 2022 meta-analysis of 381 RCTs (24,532 participants) demonstrated:-
Significant pain reduction compared to placebo (SMD = -0.96, 95% CI -1.14 to -0.78)
Effect maintained across different pain conditions and methodological approaches.
Minimal adverse events limited to mild skin irritation in <2% of patients.
Condition-specific evidence:
Diabetic neuropathy: High-frequency TENS showed 34.7% greater pain reduction than low-frequency TENS
Spinal cord injury: Low-frequency TENS significantly reduced VAS scores compared to sham treatment.
Fibromyalgia: Clinical trials suggest benefit, though limited by small sample sizes.
One of the challenges is that the TENS terminology is not specific in terms of the stimulation parameters, and studies will use different stimulation parameters than others. This complicates the gathering of evidence.
2. Spinal Cord Stimulation (SCS)
SCS involves epidural placement of electrodes to stimulate the dorsal columns, and is considered to represent the gold standard for many neuropathic pain conditions that do not respond well to other standard treatments. This is obviously a significant step and may be applied after trying typical medications such as gabapentin, pregabalin, antidepressants, or other therapies that help most people. This approach may be particularly useful when pain is widespread across multiple areas.
Mechanisms
SCS modulates pain through:
Dorsal column activation of large myelinated nerve fibres
Neurotransmitter modulation including GABA, serotonin, and endogenous opioids
Descending inhibition from brainstem pain control centers
Cortical and subcortical modulation affecting pain perception and emotional processing
Clinical Effectiveness
Success rates for SCS range from 47-74% for long-term pain relief, with significant variation by condition.
Complex Regional Pain Syndrome: >80% success rate in specialised centers
Failed Back Surgery Syndrome: 67-74% achieve >50% pain relief.
Peripheral neuropathic pain: 67.9% long-term success in comprehensive studies
Advanced SCS technologies including high-frequency stimulation, burst stimulation, and dorsal root ganglion stimulation show promise for enhanced outcomes.
3. Peripheral Nerve Stimulation (PNS)
PNS targets specific peripheral nerves through percutaneous electrode placement, offering advantages over SCS for focal neuropathic conditions where the nerve pain is localised and restricted to one region of the body.
Clinical Evidence
Recent systematic reviews demonstrate:
67% of patients with peripheral neuropathic pain achieve ≥50% sustained pain relief
Long-term effectiveness maintained up to 16 years in case series
Superior safety profile compared to SCS with no risk of central cord injury
High-quality evidence includes randomised controlled trials showing 58-67% responder rates for conditions such as post-amputation pain and complex regional pain syndrome.
Successes of Electrical Stimulation
Documented Effectiveness
TENS demonstrates consistent benefits:
Moderate-certainty evidence for pain reduction across multiple conditions
Number Needed to Treat of 3.3 for clinically meaningful pain reduction in fibromyalgia
Prolonged efficacy when combined with standard drug therapy, extending benefits by 31% for up to 6 months.
However, remember that TENS is not just one thing, and various forms of application and stimulation parameters are being used.
SCS shows robust long-term outcomes:
70% trial-to-implant success rates in contemporary studies.
Sustained pain relief with mean Visual Analogue Scale score (VAS) improvement of 61.4% at 12.85 months follow-up
Quality of life improvements including reduced disability, improved mood, and decreased healthcare utilisation.
PNS provides targeted relief:
Two-thirds success rate for peripheral neuropathic conditions
Enduring benefit with 80% of patients maintaining ≥50% pain relief at long-term follow-up.
A percutaneous procedure involves inserting electrodes through the skin rather than by open surgery. This means that electrodes can be placed close to a peripheral nerve. And of course, the technique is minimally invasive compared to traditional surgery.
Advantages Over Pharmacological Treatment
Electrical stimulation offers several benefits:
Non-systemic approach avoiding drug-related side effects and interactions. Many patients would avoid taking drugs if they can.
Adjustable therapy allowing parameter optimisation for individual patients
Long-term cost-effectiveness despite higher initial investment.
Preserved cognitive function without sedation or mental clouding that can result from some drug-based therapies.
Reduced opioid dependence potential in comprehensive pain management
Limitations and Complications
TENS Limitations
Clinical limitations include:
Variable response rates with significant inter-individual differences in effectiveness
Short-term effects requiring repeated applications for sustained benefit
Analgesic tolerance development with repeated use at identical parameters
Limited effectiveness for certain neuropathic conditions, particularly central pain syndromes
Contraindications and precautions:
Cardiac pacemakers when present, represent a contraindication due to potential electromagnetic interference
Pregnancy when applied over abdomen or pelvis.
Epilepsy requiring careful electrode placement away from head and neck
Skin conditions including broken skin, irritation, or diminished sensation
These contra-indications and precautions are typical of pretty much all forms of electrical stimulation.
SCS Limitations and Complications
Technical complications:
Hardware failures including lead migration (13.9%), breakage (6.7%), and device malfunction (17.8%)
Infection rates requiring system removal in some cases
Need for revision surgery for battery replacement or lead repositioning
Clinical limitations:
Variable success rates particularly for central neuropathic pain conditions
Patient selection challenges with 26-30% experiencing inadequate long-term benefit
Limited effectiveness for spinal cord injury pain, with only 25% achieving satisfactory relief in some series of research study.
Economic considerations:
High initial costs for device implantation and trial procedures
Ongoing maintenance requirements including battery replacements and programming adjustments
Cost-effectiveness dependent on long-term success and reduced alternative treatment needs
As we will see below, these limitations and complications may be avoided in many cases by the adoption of transcutaneous spinal cord stimulation methods (tSCS)
PNS Limitations
Technical challenges:
Lead placement difficulties particularly in anatomically complex regions
Limited battery life in non-rechargeable systems requiring replacement every 2-5 years
Risk of lead migration or displacement affecting therapeutic efficacy
Clinical considerations:
Focal application limiting usefulness for widespread pain conditions
Variable response with some patients experiencing diminishing benefits over time
Limited long-term data for newer PNS systems and techniques
Future Directions and Considerations
Technological Advances
Emerging technologies show promise for improving electrical stimulation outcomes:
Closed-loop systems providing automatic adjustment based on physiological feedback. Whereas traditional electrical stimulation devices deliver preset stimulation regardless of changing patient needs or responses, closed-loop systems can use real-time feedback from the patient. This might include signals such as nerve activity, EMG or pain markers and then use this information to automatically adjust the stimulation settings. The aim would be to provide a more personalised and responsive type of therapy. We can imagine this reducing the risk of over-stimulation and thereby improving comfort while maintaining effectiveness.
Novel waveforms including differential target multiplexed and fast-acting subperception therapy. Basic stimulators that use the TENS approach have often used quite simple stimulation patterns of single-phase or biphasic pulse patterns. Of course, other patterns such as burst stimulation, very high frequency pulses, or complex pattern signals are also possible. These may well be better at blocking pain signals or reducing tolerance. For example, burst stimulation attempts to mimic natural nerve firing. The idea is to trick the nervous system in new ways to reduce pain more efficiently and effectively.
Improved electrode designs for enhanced targeting and reduced complications. When using electrical stimulation, it is electrodes that deliver the current to the nerves or spinal segments. It's always a challenge to use electrodes and provide the right precision. When surface electrodes are used, tissue reactions can occur in some cases. Thin-film or flexible electrodes are under consideration that would be smaller, allow more focus targeting, and potentially improved biocompatibility. Arrays of electrodes with multiple stimulation zones may be deployed.
Wireless power transmission eliminating implanted battery requirements. For SCS, internal batteries may be required, which can wear out, resulting in the need for replacement surgery. Wireless power transmission could use external sources to power these implants. Energy from outside of the body could be transmitted via radio frequencies, ultrasound, or induction, eliminating the need for surgeries.
Personalised Medicine Approaches
Research directions include:
Biomarker identification for patient selection and outcome prediction. Biomarkers are measurable biological signals that could give information about the status of the condition or the individual's response to treatment. We can imagine that in this case of neuropathic pain, identifying suitable biomarkers could help predict who will best respond to electrical stimulation. It could also help with the selection of stimulation parameters and give an indication of treatment progress.
Genetic testing to identify responders to specific stimulation modalities. Certain Genetic traits may mean a person is, for example, more sensitive to electrical stimulation, is at a higher or lower risk of complications.
Advanced imaging for optimal electrode placement. High-resolution scans could be used to map individual nerve pathways and pain sources. This could help clinicians visualise nerve damage and precisely guide the placement of electrodes. For example, it might be possible to use functional MRI to identify the spinal cord segment most responsible for pain, thereby allowing a more precisely tailored electrode placement.
Machine learning algorithms for parameter optimisation. The acceleration of interest in machine learning and AI offers the potential of processes that can analyse complex data such as responses to pain, biomarker profiles, and imaging data to find patterns and predict the best therapy options. The result could be software that adjusts the electrical stimulation settings automatically based on pain ratings, nerve signals and previous results.
Our Approach at Anatomical Concepts
At Anatomical Concepts, we have a lot of experience in working with electrical stimulation in its various forms. The systems we use support FES Cycling, Neuromuscular electrical stimulation applications (NMES), And less well-known applications, such as the treatment of peripheral nerve injuries and spinal cord injuries resulting in denervated muscle.
Two systems that we use which are relevant to this article and neuropathic pain are the Stim2go and the Edition 5 system from Schufried.
The Stim2Go

Stim2Go
One of our newest products, the Stim2Go from Pajunk GmbH, is a very versatile product and the heart of our FES Cycling offering these days. However, it offers much more than that.
The Stim2go is a next generation system designed for non-invasive neural rehabilitation, and it notably supports tSCS alongside other modalities like Functional Electrical Stimulation(FES), NMES, and TENS.
Deployment of tSCS with Stim2Go
tSCS with Stim2Go is used as a painless, surface-applied therapy aimed at reducing spasticity and supporting pain relief. Research is on the way to establish whether this approach can also enhance voluntary motor control, especially in people with spinal cord injury or multiple sclerosis.
The system uses a specific electrode configuration (typically three electrodes: two on the abdomen, one on the lower back at T11/12) and delivers biphasic rectangular pulses. Stim2Go's protocols do not use a high-frequency carrier, focusing instead on precise, patient-specific stimulation patterns. There is an initial tSCS priming programme available which can be used to determine the optimal current intensity. It can be used to calibrate the therapeutic settings to each individual.
The tSCS implementation allows the client to use this protocol during FES cycling, or when lying or standing. Stim2Go's tSCS programs are MDR approved in Europe (not FDA cleared in the USA at this time); no formal functional claims for tSCS are currently being made, but ongoing deployments in UK rehab environments will inform best practice.
TENS
Stim2go includes a range of TENS protocols that are designed for flexible, non-invasive pain management. Stim2go uses a template structure, and templates can be deployed as designed or they can be copied and custom versions created. The templates are evidence-based, pre-set routines. Custom versions of these allow adjustment of:
Pulse frequency
Pulse width
Intensity
Pattern of stimulation
The standard included protocols are :-
"Conventional" (High-Frequency) TENS: Fast pulses (often 80–120 Hz) with low-medium intensity; These produce a comfortable, tingling sensation designed to block pain signals at the spinal cord level (“gate control theory”).
Low-Frequency (Acupuncture-Like) TENS: Slower pulses (2–10 Hz), often stronger intensity; may promote release of endogenous opioids and deliver longer-lasting analgesia.
Burst Mode: Pulses grouped into “bursts” at intervals, blending features of conventional and low-frequency for some users.
The Stim2Go is proving popular for this use case because users and clinicians can easily adjust the parameters or build a completely individualised protocol using the app interface. The programmes are single- or multi-channel, which can allow targeting of multiple body regions.
The Video below from Pajunk’s YouTube channel nicely shows one method of using Stim2go for pain relief.
The Edition 5

Edition 5, 2-channel electrical stimulation device.
The Schufried Edition 5 (Stimulette Edition 5 S2x) is a highly versatile electrotherapy device that offers one of the broadest selections of pain-relieving stimulation waveforms available in clinical electrotherapy. Here’s a summary of its approach to pain stimulation:
Pain Waveforms Supported
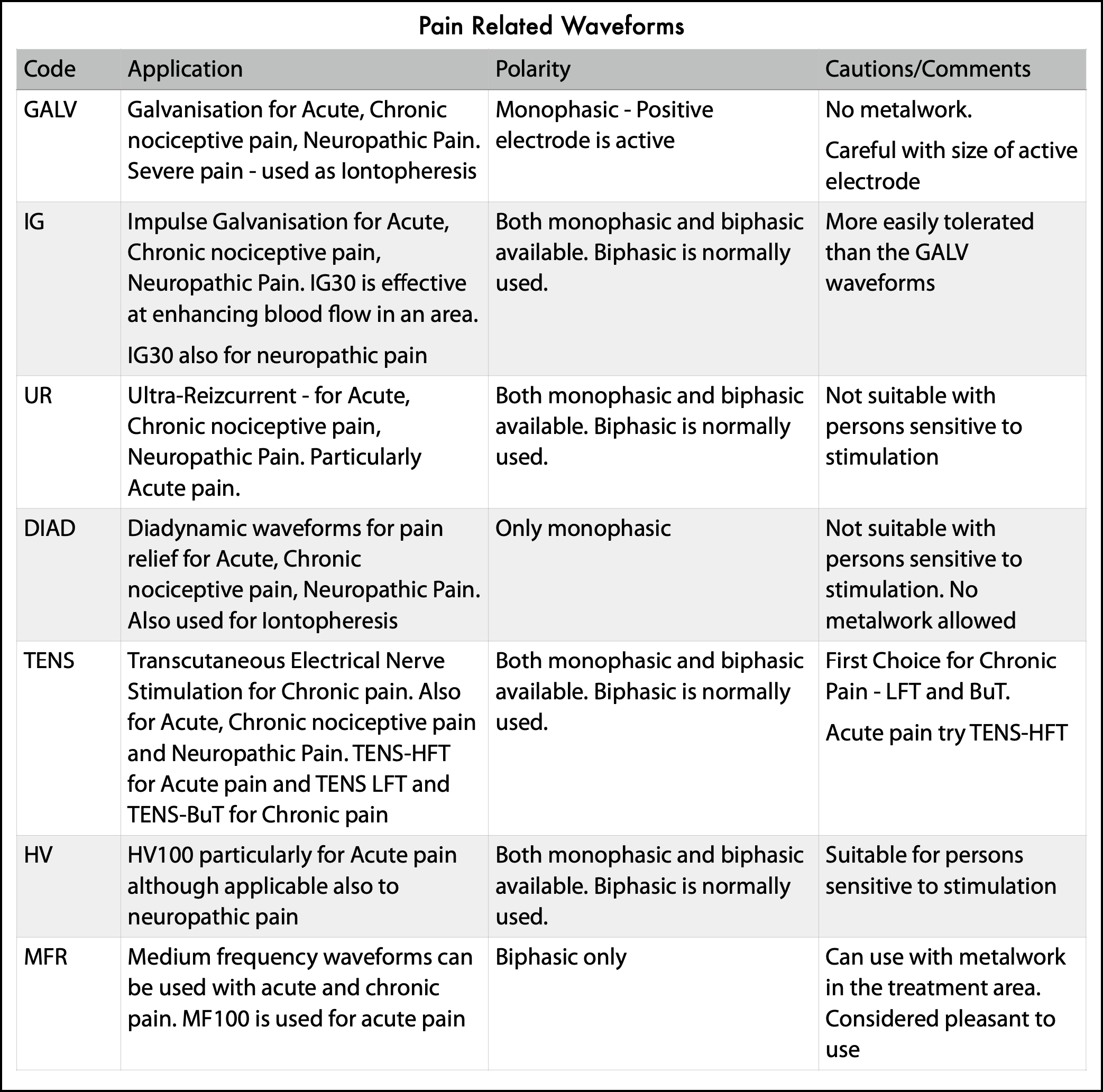
1. Galvanisation (GALV) Waveforms:
Monophasic direct current in three intensities (GALV10, GALV25, GALV50).
Indications: Acute, chronic nociceptive pain, neuropathic pain, pre-treatment (to enhance response to other waveforms), and iontophoresis.
2. Impulse Galvanisation (IG) Waveforms:
IG30 (lower frequency, 13 Hz): Vasodilation, analgesia, useful for neuropathic and chronic pain.
IG50 (higher frequency, 185 Hz within 8 Hz bursts): Quick, longer-lasting analgesia.
Biphasic variants
3. Ultra-Reizcurrent (UR) Waveform:
Interrupted direct current, known as “ultra-stimulation” or Trabert current.
Biphasic preferred. Best for acute and chronic pain (nociceptive and neuropathic).
Quickly raises pain threshold via gate control, often used for whiplash and similar acute injuries.
4. Diadynamic (DIAD) Waveforms:
Four variants, popular in various regions for alternating current-based pain relief.
5. TENS Waveforms:
TENS-LFT: Low-frequency (opioid-mediated), stimulates A-delta fibers; slower-acting but long-lasting effect, good for chronic and neuropathic pain.
TENS-HFT: High-frequency (80–120 Hz, pain gate mechanism, A-beta fibers); fast effect for acute pain.
TENS-BuT: Burst mode, pulses delivered in bursts, stimulates both gate control and opioid systems at once.
6. High Voltage (HV) Waveform:
HV100: Preferred for acute pain, particularly for patients sensitive to other types of stimulation.
7. Medium Frequency (MF) Waveforms:
MF100: Sinusoidal, 100 Hz amplitude modulation; pain-blocking via gate control, suitable for acute and chronic nociceptive pain, and for sensitive patients.
Not all of the pain-oriented waveforms above are suitable for neuropathic pain and some of these waveforms are relatively unknown in the United Kingdom.
It is quite often necessary to apply trial and error over a period of time to find the most suitable waveform for pain relief. Our starting point will typically be the TENS waveforms within the Edition 5 system.
Conclusions
Electrical stimulation represents a valuable therapeutic option in the comprehensive management of neuropathic pain, offering non-pharmacological alternatives for patients with inadequate response to conventional treatments.
TENS provides accessible, low-risk intervention with moderate-certainty evidence for effectiveness, while SCS and PNS offer more intensive options for refractory cases with demonstrated long-term benefits in appropriately selected patients.
Success rates vary significantly by condition and patient factors, with peripheral neuropathic pain generally responding better than central pain syndromes.
Complications are generally manageable but require specialised expertise and careful patient selection to optimise outcomes.

Versatile Stim2Go
The integration of electrical stimulation into comprehensive pain management programs, combined with pharmacological treatments, physical therapy, and psychological interventions, offers the best approach for addressing the complex, multifaceted nature of neuropathic pain conditions.
For rehabilitation professionals in the NHS system, electrical stimulation modalities represent evidence-based treatments that can significantly improve patient outcomes when appropriately selected and implemented within comprehensive care pathways.
At Anatomical Concepts, the Stim2go offers a versatile approach for many situations as the device can be used in many ways to support rehabilitation. It's incorporation of tSCS is an exciting It is an exciting benefit for many users who find that this can give greater control over troublesome spasticity and pain. tSCS can be combined with FES cycling.
Where denervation is an issue, perhaps due to a peripheral nerve injury or spinal cord injury, the Edition 5 may well be our preferred choice, due to the wide variety of programmes available to support both pain relief and denervation.
Neuropathic pain remains difficult to treat, and success can be uncertain. The advantage of electrical stimulation is that the variety of methodologies can be tried with little risk and much to gain.